Received: Mon 19, May 2025
Accepted: Thu 29, May 2025
Abstract
Introduction: Vasoplegic syndrome after cardiac surgery with cardiopulmonary bypass (CPB) is a frequent complication that is associated with significant morbidity and mortality. The aim of this study was to identify predictive biomarkers of vasoplegic syndrome on the first postoperative day (POD 1) following cardiac surgery with CPB among three immune signal effector proteins, Syk, PLC-G and SHP-1, in monocytes and neutrophils.
Methods: Patients undergoing cardiac surgery with scheduled CPB without autoimmune disease or preoperative infection were included. The expression of phosphorylated Syk, PLC-G and SHP-1 in monocytes and neutrophils was measured by flow cytometry prior to (T0) and after (T1) CPB on PODs 1, 3 and 7. Associations between norepinephrine (NOR) use on POD 1 and protein fluorescence at T1 or T1/T0 ratios were assessed.
Results: Of the 23 patients analysed, four (17%) had NOR on POD 1. No association was found between NOR on POD 1 and the expression of the studied proteins at T1. The T1/T0 ratio of Syk in monocytes was lower in patients without NOR on POD 1 (p=0.032). The area under the ROC curve for this marker was 0.85 [0.60-1.00]. The value of 0.47 provided a sensitivity of 1 and a specificity of 0.74.
Conclusion: Phosphorylation status of Syk in monocytes is a predictive biomarker for the occurrence of vasoplegic shock following cardiac surgery with CPB.
Keywords
Cardiac surgery, cardiopulmonary bypass, vasoplegic, shock inflammation, SYK
1. Introduction
Despite the progress made in recent years, cardiac surgery with cardiopulmonary bypass (CPB) is still associated with significant morbidity and mortality rates [1]. Enhanced recovery after surgery protocols have been implemented in many surgical specialties, including cardiac surgery [2]. These programs reduce postoperative complications and length of stay and control costs [3, 4]. However, the presence of postoperative shock contraindicates some early rehabilitation measures and limits their benefits.
One of the main causes of postoperative shock following cardiac surgery with CPB is vasoplegic syndrome, which can be associated with organ failure, such as acute kidney injury. This results in an important inflammatory response generated by the surgical stimulus and the CPB itself [5]. Blood perfusion in the CPB circuit leads to the activation of immune cells [6]. Neutrophils and monocytes are the primary effectors of this inflammatory response. Monocyte activation results in the secretion of cytokines, and neutrophil activation leads to extracellular release of cytotoxic molecules and reactive oxygen species that lyse the extracellular matrix and epithelial cell junctions, resulting in increased vascular permeability, microthrombi formation and parenchymal cell injury [7]. The main immunoreceptors of both monocytes and neutrophils are the receptors for the constant region of antibodies, the Fc receptors (FcRs). Activation of FcRs, through the recognition of their ligands, triggers signalling cascades leading to modulation of the inflammatory response [8]. They can induce an activating signal (ITAMa) by the phosphorylation of the Syk protein that leads to the phosphorylation of the PLC-G protein or an inhibiting signal via the phosphorylation of the SHP-1 protein (ITAMi).
A better understanding of the activation of these phagocytic cells could help physicians better understand the inflammatory response and its complications after cardiac surgery. Many predictive biomarkers have been described in cardiac surgery [9-11]. However, few studies have investigated the activation status of these immune cells. The aim of this study was to identify predictive biomarkers of vasoplegic syndrome on the first postoperative day (POD 1) following cardiac surgery with CPB that could be used in daily practice and could help physicians select patients for early rehabilitation measures or for early haemodynamic optimization measures.
2. Patients and Methods
2.1. Study Design
This prospective, monocentric, proof of concept and observational research study was performed according to current guidelines in a tertiary care teaching hospital performing more than 1,000 annual cardiac surgical procedures with CPB.
Between June 1st and September 30th, 2019, all patients hospitalized for cardiac surgery with CPB scheduled on a Tuesday morning were eligible. For reasons of technical feasibility related to the sampling schedule, only two patients per week could be included on Tuesday morning. This allowed each blood sample to be processed immediately after collection on working days. The non-inclusion criteria were preoperative infection, long-term immunosuppressive therapy (corticosteroids), incompetent patients, minor patients, and patient refusal to participate in the study. Patients in whom immunological markers were not assessed at the end of CPB were also not included.
2.2. Objectives
The primary endpoint was to identify a predictive marker at the end of surgery that identified the need for norepinephrine (NOR) on POD 1 among three proteins mediating monocyte and neutrophil FcR signalling: SHP-1, Syk and PLC-G. Secondary endpoints were to evaluate the evolution of the phosphorylation of SHP-1, Syk and PLC-G during the first 7 POD to evaluate the association with blood cytokine secretion.
2.3. Data Collection
2.3.1. Clinical Data
Clinical data were prospectively collected on PODs 0, 1, 3 and 7.
2.3.2. Biological Data
Blood collections scheduled for the study were as follows. The first blood sample was collected after anaesthetic induction and before any surgical stimulus. It was used to evaluate the baseline value of each marker. Then, blood samples were obtained at the end of CPB (T1), on the morning of POD 1 (T2), on the morning of POD 3 (T3) and finally on the morning of POD 7 (T4). T0 and T1 blood samples were collected during the pre- and post-CPB biological analyses, respectively. T2, T3, and T4 blood samples were collected between 6 and 7 a.m. during the morning blood tests performed as part of the patient's standard management.
Samples were then sent to the immunology laboratory for analysis by flow cytometry. The manipulations were performed on whole blood. Monocytes and neutrophils were identified by flow cytometry via FSC/SCC (forward scatter/side scatter) and CD14/CD16. After permeabilization, labelling of intracellular proteins was performed using fluorescent antibodies specific to the phosphorylated forms of the three proteins studied: pSHP-1S591, pSykY525 and pPLC-GY759 (Supplementary Material). These phosphorylations activate Syk and PLC-G, whereas they inhibit SHP-1. The levels of phosphorylation were expressed as the mean fluorescence intensity.
2.4. Patient Management
2.4.1. Anaesthesia Management
The anaesthetic management of patients was standardized and independent of the type of surgery performed. Patient monitoring included measurements of invasive arterial pressure, central venous pressure, and depth of anaesthesia by bispectral index (BIS) and the use of transesophageal echocardiography. Induction and maintenance were performed with propofol and sufentanil administered by target-controlled infusion. The hypnotic component of anaesthesia was titrated aiming to maintain BIS values between 40 and 60. Muscular relaxation was achieved by repeated boli of atracurium. Tranexamic acid was administered after induction by bolus and continuous infusion. No locoregional analgesia was performed. The transfusion of labile blood products was conducted according to protocol.
2.4.2. Cardiopulmonary Bypass Management
CPB was performed in normothermia and with myocardial protection by intermittent anterograde or retrograde warm blood cardioplegia. Venous cannulation was atrio-cava or of both vena cava and arterial cannulation at the ascending thoracic aorta. A bolus of 300 IU/kg unfractionated heparin was administered before the initiation of CPB for an ACT (activated clotting time) target of > 400 seconds. At the end of the procedure, dose-for-dose protamine antagonization was performed to achieve an ACT below 120% of the basal value. Phenylephrine boli were administered to maintain a mean arterial pressure between 60 and 80 mmHg before and during CPB. Venous line oxygen saturation > 80% was targeted. Norepinephrine (NOR) vasopressor support was instituted intraoperatively in case of repeated use of phenylephrine. Inotropic support was initiated according to anaesthetist or intensivist discretion. Non-heparin-bonded circuits were used. Haemofiltration during CPB was not performed systematically. Fluid therapy was at the discretion of the perfusionist to allow the delivery of a flow consistent with the theoretical cardiac output calculated according to the patient's weight and height.
2.4.3. Postoperative Care Management
All patients were admitted to the cardiac surgery intensive care unit (ICU) immediately after surgery. NOR was administered when the mean arterial pressure was below 65 mmHg despite adequate fluid resuscitation. Propofol sedation initiated in the operating room was continued in the ICU and then stopped for extubation. Extubation took place between 4 and 6 hours after admission unless the patient had immediate postoperative respiratory, haemodynamic, or haemorrhagic complications that contraindicated it. Preventive anticoagulation with unfractionated heparin was started after 6 hours in the absence of bleeding complications. Postoperative analgesia was according to protocol: paracetamol and nefopam intravenously followed by oral administration and morphine subcutaneously after initial intravenous titration. Insulin therapy was administered intravenously for the first 24 hours and then subcutaneously. All patients received motor and respiratory physiotherapy the day after surgery. Drains were removed at the 36th hour after the surgery.
2.5. Ethics Approval
The written and signed consent of the patients was collected after providing them with oral and written information the day prior to surgery. The protocol received favourable approval from the institutional review board “Comité de protection des personnes Est I” (ID-RCB: 2018-A00216-49). The collected data were declared to the Commission Nationale de l’Informatique et des Libertés (CNIL, declaration number 2191694v0).
2.6. Statistical Analysis
Continuous variables are expressed as median values with interquartile ranges [IQRs] and were compared with the Mann-Whitney U test or the Kruskal-Wallis test as appropriate. Categorical variables are expressed as counts and percentages and were compared with Fisher’s exact test or the chi-square test, as appropriate. Patients were separated into two groups according to the prescription of NOR on POD 1 and the level of the Syk T1/T0 ratio in monocytes. Receiver operating characteristic (ROC) curves were generated to explore the sensitivity and specificity of the markers to predict the prescription of NOR on POD 1, and the Youden index was calculated to determine the best threshold value. Statistical and graphical analyses were performed with R software v4.0.3 (Link 1). A p value < 0.05 was considered statistically significant.
3. Results
3.1. Patient Characteristics
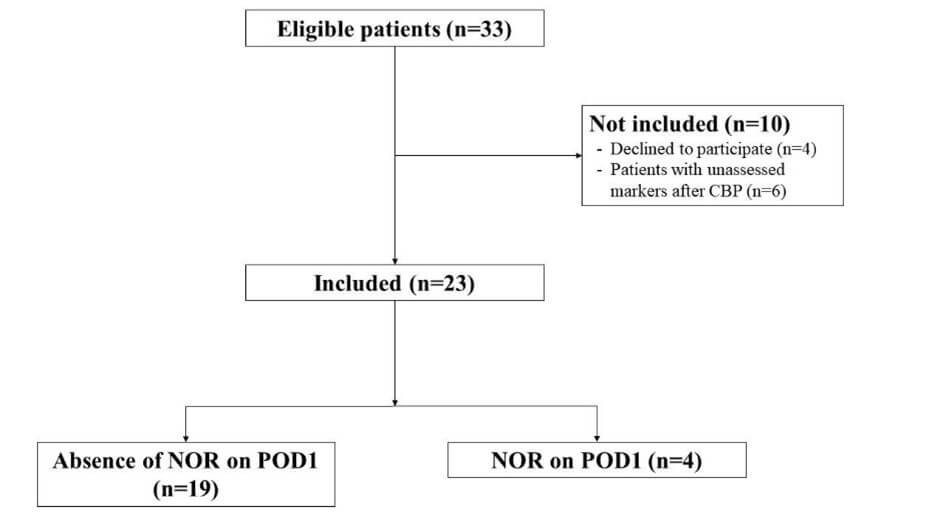
Between June 1st and September 30th, 2019, 33 patients were eligible, 23 of whom were included and analysed. Of these, four patients (17%) received NOR on POD 1 (Figure 1). These patients were less likely to have undergone coronary artery bypass graft surgery (CABG) (25% vs. 79%, p = 0.008), they had longer aortic cross clamping and CPB duration (respectively 82 min [79-118] vs. 40 min [33-47] and 106 min [100-167] vs. 49 min [39-57], both p=0.003), and they had longer lengths of ICU stay (16 days [8.5-27] vs. 3 [2-3.5], p = 0.004). Notably, these patients had more biological abnormalities on POD 1 with more elevated creatinine and lactate levels and lower platelet counts and haemoglobin levels (Table 1).
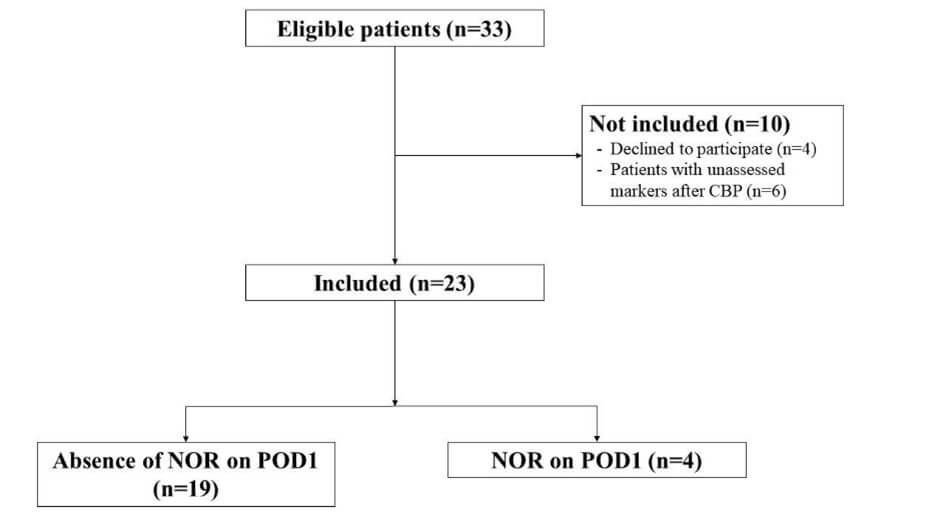
NOR: Norepinephrine; POD: Postoperative day.
TABLE 1: Characteristics of the study population according to norepinephrine
infusion on the first postoperative day.
|
Variables |
All patients n = 23 |
Patients
without NOR on POD 1 n = 19 |
Patients with
NOR on POD 1 n = 4 |
p |
|
Clinical characteristics |
|
|||
|
Age (years) |
68 [56-73] |
68 [58-73] |
54 [36-73] |
0.52 |
|
Male gender |
17 (74) |
14 (74) |
3 (75) |
1.00 |
|
Body mass index |
27 [23-29] |
27 [25-30] |
23 [22-23] |
0.02 |
|
Hypertension |
15 (65) |
13 (68) |
2 (50) |
0.59 |
|
Dyslipidaemia |
11 (48) |
11 (58) |
0 |
0.09 |
|
Diabetes |
7 (30) |
7 (37) |
0 |
0.27 |
|
LEAOD |
2 (9) |
2 (11) |
0 |
1.00 |
|
LVEF < 50% |
4 (17) |
3 (16) |
1 (25) |
1.00 |
|
ACE inhibitor |
12 (52) |
11 (58) |
1 (25) |
0.32 |
|
Statin |
14 (61) |
13 (68) |
1 (25) |
0.26 |
|
Beta blocker |
19 (83) |
17 (90) |
2 (50) |
0.12 |
|
EuroSCORE II |
1.4 [1.1-3.5] |
1.2 [1.0-2.0] |
7.4 [6.4-9.5] |
0.005 |
|
Surgery |
|
|||
|
Prior cardiac surgery |
2 (9) |
0 |
2 (50) |
0.02 |
|
CABG |
16 (70) |
15 (79) |
1 (25) |
0.008 |
|
Valvular surgery |
7 (30) |
4 (21) |
3 (75) |
0.07 |
|
Aortic valve replacement |
5 (22) |
3 (16) |
2 (50) |
0.19 |
|
Mitral valve replacement |
2 (9) |
1 (5) |
1 (25) |
0.32 |
|
Aortic surgery |
1 (4) |
0 |
1 (25) |
0.17 |
|
Aortic cross-clamping duration (minutes) |
43 [35-53] |
40 [33-47] |
82 [79-118] |
0.003 |
|
CPB duration (minutes) |
50 [41-72] |
49 [39-57] |
106 [100-167] |
0.003 |
|
Transfusion |
6 (26.1) |
3 (16) |
3 (75) |
0.04 |
|
Postoperative data |
|
|||
|
Catecholamines at the end of CPB |
14 (61) |
10 (53) |
4 (100) |
0.13 |
|
Norepinephrine alone |
9 (39) |
8 (42) |
1 (25) |
1.0 |
|
Dobutamine alone |
1 (4) |
0 |
1 (25) |
0.17 |
|
Norepinephrine and dobutamine |
4 (17) |
2 (11) |
2 (50) |
0.12 |
|
Surgical site bleeding (mL) |
805 [585-1135] |
850 [565-1155] |
660 [645-745] |
0.47 |
|
Mechanical ventilation on POD 1 |
1 (4) |
0 |
1 (25) |
0.17 |
|
Postoperative atrial fibrillation |
4 (17) |
3 (16) |
1 (25) |
1.00 |
|
Postoperative AKI |
3 (13) |
1 (5) |
2 (50) |
0.07 |
|
ICU length of stay (days) |
3.0 [2.0-5.0] |
3.0 [2.0-3.5] |
16.0 [8.5-27.0] |
0.004 |
|
Blood parameters on POD 1 |
||||
|
Leukocyte count (G/L) |
11.1 [9.7-13.0] |
11.4 [10.3-13.2] |
9.7 [8.2-10.6] |
0.19 |
|
Platelet count (G/L) |
173 [158-222] |
186 [162-228] |
149 [127-162] |
0.039 |
|
Haemoglobin (g/dL) |
11.6 [10.6-12.2] |
11.7 [11.2-12.4] |
8.9 [8.3-10.1] |
0.028 |
|
Blood lactate level (mmol/L) |
1.3 [1.1-1.7] |
1.3 [1.1-1.5] |
2.0 [1.7-3.5] |
0.025 |
|
Creatinine level (µmol/L) |
77 [64-114] |
73 [59-95] |
129 [114-160] |
0.021 |
|
Potassium (mmol/L) |
4.5 [4.0-4.9] |
4.3 [3.9-4.7] |
5.0 [4.9-5.1] |
0.039 |
|
Troponin (µg/L) |
3 [2-6] |
3 [2-4] |
21 [16-191] |
<0.001 |
|
AST (UI/L) |
36 [29-57] |
34 [28-42] |
83 [59-262] |
0.06 |
|
AST (UI/L) |
36 [29-57] |
34 [28-42] |
83 [59-262] |
0.06 |
Continuous variables are expressed as the median and interquartile range
[IQR] and were compared using the Mann-Whitney U test. Categorical variables
are expressed as n (%) and were compared with Fisher’s exact test.
NOR: Norepinephrine; POD: Postoperative day; LEAOD: Lower Extremity Arterial Occlusive Disease; LVEF: Left Ventricular Ejection Fraction; ACE: Angiotensin-Converting Enzyme; CABG: Coronary Artery Bypass Grafting; CPB: Cardiopulmonary Bypass; AKI: Acute Kidney Injury; AST: Aspartate-Aminotransferase; ICU: Intensive Care Unit.
3.2. Descriptive Evolution of Phosphoprotein Fluorescence Intensity
The evolution of the intensity of the three proteins studied was very different between neutrophils and monocytes. First, it should be noted that the intensity of the fluorescence in the basal (induction, T0) state was spread across a large scale, with the maximum intensity for each protein being at least 10 times superior to that of the minimal intensity (Figure 2). Second, the median fluorescence in monocytes was at least ten times higher than the fluorescence in neutrophils. Third, no general pattern can be deciphered with respect to the evolution of phosphorylation during the first week after surgery. Nevertheless, it should be noted that at the end of CPB (T1), the fluorescence of SHP-1 and PLC-G in neutrophils and Syk and PLC-G in monocytes showed a significant reduction in phosphorylation compared to T0. This decrease in phosphorylation in neutrophils and monocytes suggests a reduction in the activation of these cells.
3.3. Identification of a Marker of Norepinephrine Requirement on POD 1
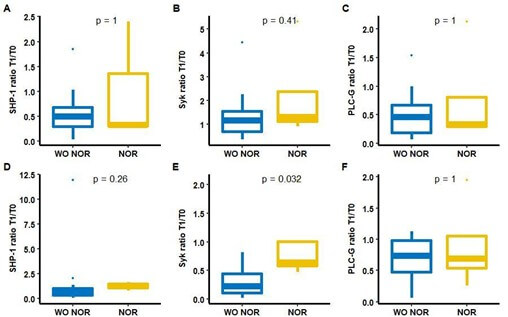
Absolute fluorescence intensities of the three proteins studied at T1 in both monocytes and neutrophils were not different between patients receiving NOR on POD 1 and those free of NOR (Figure 3). Of the six ratios of proteins studied in both neutrophils and monocytes, only the Syk ratio in monocytes differed depending on whether patients received NOR on POD 1. Indeed, the T1/T0 fluorescence Syk ratio in monocytes was lower in patients not receiving NOR on POD 1 than in those receiving NOR, with respective values of 0.22 [0.11-0.45] and 0.64 [0.58-1.01] (p=0.032). (Figure 4).
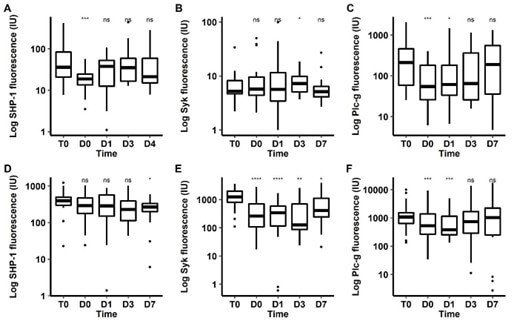
A, B, C) Fluorescence in neutrophils. A) SHP-1, B) Syk, C) PLC-G.
D, E, F) fluorescence in monocytes. D) SHP-1, E) Syk, F) PLC-G.
T0, induction; T1, end of cardiopulmonary bypass; T2, POD 1; T3, POD 3; T4, POD 7.
The p value refers to the paired comparison according to the Wilcoxon test for paired samples between T0 and T1/T2/T3/T4.
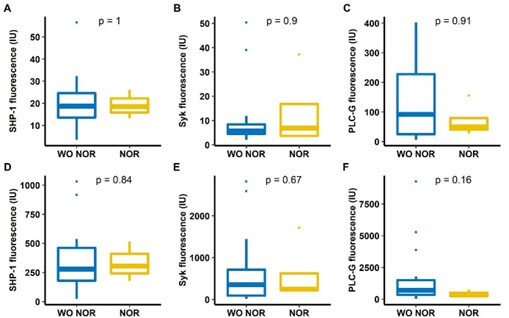
A, B, C) fluorescence in neutrophils. A) SHP-1, B) Syk, C) PLC-G.
D, E, F) fluorescence in monocytes. D) SHP-1, E) Syk, F) PLC-G.
NOR: Noradrenaline; PLC-G: Phospholipase C Gamma; SHP-1: Src Homology 2 Domain-Containing Phosphatase 1; Syk: Spleen Tyrosine Kinase; WO NOR: Without Noradrenaline.
A, B, C) fluorescence in neutrophils. A) SHP-1, B) Syk, C) PLC-G.
D, E, F) fluorescence in monocytes. D) SHP-1, E) Syk, F) PLC-G.
T0: Induction of anaesthesia, T1: end of CPB.
NOR: Noradrenaline; PLC-G: Phospholipase C Gamma; SHP-1: Src Homology 2 Domain-Containing Phosphatase 1; Syk: Spleen Tyrosine Kinase; WO NOR: Without Noradrenaline.
This Syk ratio in monocytes was correlated with the SHP-1 ratio in monocytes (rho = 0.64, p = 0.025) but was not correlated with the Syk ratio in neutrophils (rho = 0.28, p = 0.19) (Supplementary Figure 1). The ROC curve of the T1/T0 fluorescence Syk ratio in monocytes as a predictive marker of NOR requirement at POD 1 was generated (Figure 5). The area under the curve was 0.85 [0.60-1.00]. The value of the T1/T0 fluorescence Syk ratio allowing the best sensitivity/specificity couple was 0.47. This value was associated with a sensitivity of 1 and a specificity of 0.74. To assess the ability of this threshold to discriminate patients by outcome, patients were separated into two groups based on the value of the T1/T0 Syk fluorescence ratio in monocytes (Table 2). Patients with a ratio greater than 0.47 had longer aortic cross-clamping and CPB durations and longer length of ICU stay than those with a value less than 0.47 (57 [43-79] vs. 39 [32-46] p = 0.01, 75 [53-105] vs. 47 [39-52] p = 0.02 and 16.0 [8.5-27.0] vs. 3.0 [2.0-3.5] p = 0.004, respectively). This was also associated with more biological alterations on POD 1. Patients with a Syk ratio > 0.47 had higher creatinine, blood lactate, and aspartate-aminotransferase (AST) levels than patients with a Syk ratio < 0.7. Interestingly, these patients with a high Syk ratio had a similar proportion of catecholamine requirement to patients with a low ratio at the end of CPB (67% vs. 57%, p = 1), whereas no patient received NOR on POD 1 in the group with a low Syk ratio.
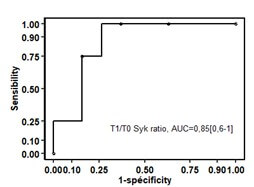
ROC: Receiver Operating Characteristic; NOR: Norepinephrine; POD: Postoperative day; AUC: Area Under the Curve; CPB: Cardiopulmonary Bypass.
4. Discussion
4.1. Summary of the Main Results
This prospective study shows that the phosphorylated forms of SHP-1, Syk, and PLC-G proteins in monocytes and neutrophils express different patterns over time after cardiac surgery with CPB. Surprisingly, the immediate post-CPB measures show low activation of monocytes with low activator phosphorylation of Syk and PLC-G (two activator proteins) and low inhibitor phosphorylation of SPH-1 (an inhibitor protein). However, no absolute fluorescence after CPB was associated with NOR on POD 1. This was linked with significant heterogeneity between patients in the basal state. Therefore, we focused on the T1/T0 Syk ratio in monocytes, which appeared to be a prognostic marker of NOR requirement on POD 1. When the population was separated according to this monocyte Syk ratio, the group with a high ratio had a greater requirement for NOR on POD 1, higher creatinine, blood lactate and AST levels and longer length of ICU stay.
4.2. Added Value of the Study
The threshold value of 0.47 yielded a sensitivity of 100% and therefore offered the possibility to select all patients requiring NOR at POD 1. The group of patients with a Syk ratio superior to this cut-off value appears to exhibit more severe condition with more biological alterations. Interestingly, this marker was not associated with NOR use at the end of CPB. Therefore, at the end of CPB, this biomarker could be used to determine which patients with NOR would have a short NOR infusion time and could then be eligible for enhanced recovery measures. Therefore, the primary application of interest of this new marker is to select patients who can benefit on the first day of central venous catheter removal, from a first rise and discharge from intensive care, which is still often the case on POD 2.
4.3. Comparison with other Studies and Physiopathological Hypotheses
4.3.1. Phosphoprotein and Vasoplegic Shock
Our hypothesis was that proteins of the signalling pathway of FcR, the most present immunoreceptors of monocytes and neutrophils, could be involved in postoperative vasoplegic shock. This complication occurs after 10-50% of CPB instances and is associated with poor outcomes as well as longer length of hospital stay [12-15]. Many factors contribute to and can explain the occurrence of vasoplegic shock after CPB, but its immunological pathophysiology remains poorly understood [16]. The fact that the expression of the studied activated proteins tended to decrease immediately after CPB, whereas the NOR requirement appeared, suggests that the role of their phosphorylation level is limited in the occurrence of vasoplegic shock. Furthermore, no association was noted at the end of CPB between the absolute phosphorylation of these proteins and the requirement for NOR on POD 1. Syk fluorescence values in monocytes after CPB were thus closer to their basal values in patients with NOR, reflecting greater activity of Syk proteins in these cells. Syk is a tyrosine kinase that mediates FcR signalling. It leads to the activation of multiple signalling pathways resulting in the activation of phagocytosis, cell-mediated cytotoxicity, and production of reactive oxygen species and cytokines [17]. The greater activation of Syk in monocytes at the end of CPB may participate in the relative proinflammatory state of these patients.
4.3.2. Immunodepression following CPB
The decrease in activator phosphorylation could suggest an immunodepression state directly after surgery and could explain the increased risk of nosocomial infection after cardiac surgery [18-20]. This result is consistent with the study by Justus et al. [21], who reported that the production of cytokines by monocytes after LPS stimulation was reduced after CPB. Indeed, Syk phosphorylation favours cytokine production [22, 23]. Therefore, the level of blood proinflammatory cytokines may not be a good reflection of the activation state of monocytes. This underlines the difficulty of separating the pro- and anti-inflammatory phases after an aggression (in this case, CPB) and indicates that the classical temporality of inflammation after an injury, an initial proinflammatory phase and subsequent anti-inflammatory phase, may be irrelevant [24]. A new point of view that associates proinflammatory and anti-inflammatory signals at the same time may be more suitable [25].
4.4. Limits and Strengths
Our study has several limitations. First, the limited number of patients included in the study as well as the small number of patients with NOR on POD 1 limit the statistical power of the analysis. Therefore, larger studies are needed to validate our biomarker, and the results of the present study can be used to calculate the required sample size. Furthermore, our study was limited to cardiac surgery; however, this technique may also be beneficial in other surgical contexts such as major digestive or thoracic procedures. In these settings, enhanced recovery protocols are also recommended, and the identification of patients at risk for postoperative complications remains a critical objective.
Second, the two groups expressed differences in their initial characteristics: for example, patients requiring NOR on POD 1 had higher EuroSCOREII values. This may represent a confusion bias when interpreting the comparison of the expression of the studied proteins. However, this bias is limited by the fact that the patient-specific ratio overcomes interindividual differences.
Third, our biomarker is not routinely measured and requires numerous manipulations by a technician with several pauses. However, its dosage does not present any difficulties for an immunology technician and does not require any specific equipment except a cytometer, which is present in all haematology laboratories. The measures come from blood samples systematically collected before and after CPB. Moreover, the results can be obtained quickly, and the cost is limited. Finally, our primary outcome—the requirement for norepinephrine on postoperative day 1- is influenced by the clinical judgment of the anesthesiologist, the intensivist, and the bedside nurse. Therefore, while it is easily measurable, it may be subject to a degree of subjectivity. However, norepinephrine administration was protocolized and aligned with recent expert recommendations for the management of vasoplegic syndrome [26].
5. Conclusion
This proof-of-concept translational study identified the phosphorylation status of Syk in monocytes as a predictive biomarker for the occurrence of vasoplegic shock following cardiac surgery with CPB that may allow enhanced recovery for patients at low risk of complications. The results presented also confirm the complexity of the inflammatory response following CPB, with an early immunodepression phase concomitant with the initial proinflammatory phase. Further large-scale prospective studies in cardiac and other surgical settings are needed to validate this predictive biomarker and its utility in forecasting the feasibility of enhanced recovery strategies.
Acknowledgements
None.
Funding
This work was supported by an ARCOTOVA grant.
Competing Interests
None.
Data Availability
The datasets generated during and/or analysed during the current study are available via the link (Link 2).
Ethics Approval
The protocol received favourable approval from the institutional review board “Comité de protection des personnes Est I” (ID-RCB: 2018-A00216-49). The collected data were declared to the Commission Nationale de l’Informatique et des Libertés (CNIL, declaration number 2191694v0).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by K. Boussion, C de Tymowski. H. Flamant and M. Hurtado-Nedelec. The first draft of the manuscript was written by K. Boussion and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Abbreviations
ACE: Angiotensin-Converting Enzyme
ACT: Activated Clotting Time
CABG: Coronary Artery Bypass Grafting
CPB: Cardiopulmonary Bypass
FcR: Fc receptor
FMLP: N-Formylmethionine-Leucyl-Phenylalanine
ICU: Intensive Care Unit
IL: Interleukin
ITAM: Immunoreceptor Tyrosine-Based Activation Motif
FSC/SCC: Forward Scatter/Side Scatter
LEOAD: Lower Extremity Arterial Occlusive Disease
LPS: Lipopolysaccharide
LVEF: Left Ventricular Ejection Fraction
MCP: Monocyte Chemoattractant Protein
NOR: Norepinephrine
PLC-G: Phospholipase C Gamma
POD: Postoperative Day
SHP-1: Src Homology 2 Domain-Containing Phosphatase 1
Syk: Spleen Tyrosine Kinase
TNF: Tumour Necrosis Factor
REFERENCES
[1]
Julien Amour,
Bernard Cholley, Alexandre Ouattara, et al. « The effect of local anesthetic continuous wound
infusion for the prevention of postoperative pneumonia after on-pump cardiac
surgery with sternotomy: the STERNOCAT randomized clinical trial. “Intensive
Care Med, vol. 45, no. 1, pp. 33-43, 2019. View at: Publisher Site | PubMed
[2]
Daniel T
Engelman, Walid Ben Ali, Judson B Williams, et al. “Guidelines for
Perioperative Care in Cardiac Surgery: Enhanced Recovery After Surgery Society
Recommendations.” JAMA Surg, vol. 154, no. 8, pp. 755-766, 2019. View
at: Publisher Site | PubMed
[3]
Robert H
Thiele, Kathleen M Rea, Florence E Turrentine, et al. “Standardization of care:
impact of an enhanced recovery protocol on length of stay, complications, and
direct costs after colorectal surgery.” J Am Coll Surg, vol. 220, no. 4,
pp. 430-443, 2015. View at: Publisher Site | PubMed
[4]
Ian O Fleming,
Claire Garratt, Ranj Guha, et al. “Aggregation of Marginal Gains in Cardiac
Surgery: Feasibility of a Perioperative Care Bundle for Enhanced Recovery in
Cardiac Surgical Patients.” J Cardiothorac Vasc Anesth, vol. 30, no. 3,
pp. 665-670, 2016. View at: Publisher Site | PubMed
[5]
Florian Kraft,
Christoph Schmidt, Hugo Van Aken, et al. “Inflammatory response and
extracorporeal circulation.” Best Pract Res Clin Anaesthesiol, vol. 29,
no. 2, pp. 113-123, 2015. View at: Publisher Site | PubMed
[6]
L H Edmunds Jr
“Inflammatory response to cardiopulmonary bypass.” Ann Thorac Surg, vol.
66, no. 5 Suppl, pp. S12-S16, 1998. View at: Publisher Site | PubMed
[7]
Jakob
Vinten-Johansen “Involvement of neutrophils in the pathogenesis of lethal
myocardial reperfusion injury.” Cardiovasc Res, vol. 61, no. 3, pp.
481-497, 2004. View at: Publisher Site | PubMed
[8]
Sanae Ben
Mkaddem, Marc Benhamou, Renato C Monteiro “Understanding Fc Receptor
Involvement in Inflammatory Diseases: From Mechanisms to New Therapeutic
Tools.” Front Immunol, vol. 10, pp. 811, 2019. View at: Publisher Site | PubMed
[9]
Michael J
Domanski, Kenneth Mahaffey, Vic Hasselblad, et al. “Association of myocardial
enzyme elevation and survival following coronary artery bypass graft surgery.” JAMA,
vol. 305, no. 6, pp. 585-591, 2011. View at: Publisher Site | PubMed
[10]
Sophie
Provenchère, Clarisse Berroeta, Catherine Reynaud, et al. “Plasma brain
natriuretic peptide and cardiac troponin I concentrations after adult cardiac
surgery: association with postoperative cardiac dysfunction and 1-year
mortality.” Crit Care Med, vol. 34, no. 4, pp. 995-1000, 2006. View at: Publisher Site | PubMed
[11]
Charles
Guenancia, Abdelkader Kahli, Gabriel Laurent, et al. “Pre-operative growth
differentiation factor 15 as a novel biomarker of acute kidney injury after
cardiac bypass surgery.” Int J Cardiol, vol. 197, pp. 66-71, 2015. View
at: Publisher Site | PubMed
[12]
John G Byrne,
Marzia Leacche, Subroto Paul, et al. “Risk factors and outcomes for “vasoplegia
syndrome” following cardiac transplantation.” Eur J Cardiothorac Surg,
vol. 25, no. 3, pp. 327-332, 2004. View at: Publisher Site | PubMed
[13]
Matthew A
Levin, Hung-Mo Lin, Javier G Castillo, et al. “Early on-cardiopulmonary bypass
hypotension and other factors associated with vasoplegic syndrome.” Circulation,
vol. 120, no. 17, pp. 1664-1671, 2009. View at: Publisher Site | PubMed
[14]
K J Tuman, R J
McCarthy, C J O'Connor, et al. “Angiotensin-converting enzyme inhibitors
increase vasoconstrictor requirements after cardiopulmonary bypass.” Anesth
Analg, vol. 80, no. 3, pp. 473-479, 1995. View at: Publisher Site | PubMed
[15]
B Mets, R E
Michler, E D Delphin, et al. “Refractory vasodilation after cardiopulmonary
bypass for heart transplantation in recipients on combined amiodarone and
angiotensin-converting enzyme inhibitor therapy: a role for vasopressin
administration.” J Cardiothorac Vasc Anesth, vol. 12, no. 3, pp.
326-329, 1998. View at: Publisher Site | PubMed
[16]
Laurence W
Busse, Nicholas Barker, Christopher Petersen “Vasoplegic syndrome following
cardiothoracic surgery—review of pathophysiology and update of treatment
options.” Crit Care, vol. 24, no. 1, pp. 36, 2020. View at: Publisher Site | PubMed
[17]
Attila Mócsai,
Jürgen Ruland, Victor L J Tybulewicz “The SYK tyrosine kinase: a crucial player
in diverse biological functions.” Nat Rev Immunol, vol. 10, no. 6,
pp. 387-402, 2010. View at: Publisher Site | PubMed
[18]
Alexis Chenouard,
Cécile Braudeau, Nicolas Cottron, et al. « HLA-DR expression in neonates after cardiac surgery
under cardiopulmonary bypass: a pilot study.” Intensive Care Med Exp,
vol. 6, no. 1, pp. 1, 2018. View at: Publisher Site | PubMed
[19]
Baptiste
Gaudriot, Fabrice Uhel, Murielle Gregoire, et al. “Immune Dysfunction After
Cardiac Surgery with Cardiopulmonary Bypass: Beneficial Effects of Maintaining
Mechanical Ventilation.” Shock, vol. 44, no. 3, pp. 228-233, 2015. View
at: Publisher Site | PubMed
[20]
Paulo E Leães,
Jorge Neumann, Luiz A Jung, et al. “Lymphocyte’s activation and apoptosis after
coronary artery bypass graft: a comparative study of two membrane
oxygenators--one with and another without a venous-arterial shunt.” ASAIO J,
vol. 50, no. 6, pp. 611-618, 2004. View at: Publisher Site | PubMed
[21]
Georgia
Justus, Christoph Walker, Lisa-Maria Rosenthal, et al. “Immunodepression after
CPB: Cytokine dynamics and clinics after pediatric cardiac surgery - A
prospective trial.” Cytokine, vol 122., pp. 154018, 2019. View at: Publisher Site | PubMed
[22]
M T Crowley, P
S Costello, C J Fitzer-Attas, et al. “A Critical Role for Syk in Signal
Transduction and Phagocytosis Mediated by Fc␥ Receptors on Macrophages.” J Exp Med,
vol. 186, no. 7, pp. 1027-1039, 1997. View at: Publisher Site | PubMed
[23]
Kevin M
Dennehy, Gerben Ferwerda, Inês Faro-Trindade, et al. “Syk kinase is required
for collaborative cytokine production induced through Dectin-1 and Toll-like
receptors.” Eur J Immunol, vol. 38, no. 2, pp. 500-506, 2008. View at: Publisher Site | PubMed
[24]
Fumio Kimura,
Hiroaki Shimizu, Hiroyuki Yoshidome, et al. “Immunosuppression following
surgical and traumatic injury.” Surg Today, vol. 40, no. 9, pp. 793-808,
2010. View at: Publisher Site | PubMed
[25]
Lori F
Gentile, Alex G Cuenca, Philip A Efron, et al. “Persistent inflammation and
immunosuppression: A common syndrome and new horizon for surgical intensive
care.” J Trauma Acute Care Surg, vol. 72, no. 6, pp. 1491-1501, 2012.
View at: Publisher Site | PubMed
[26] Fabio Guarracino, Marit Habicher, Sascha Treskatsch, et al. “Vasopressor Therapy in Cardiac Surgery-An Experts’ Consensus Statement.” J Cardiothorac Vasc Anesth, vol. 35, no. 4, pp. 1018-1029, 2021. View at: Publisher Site | PubMed